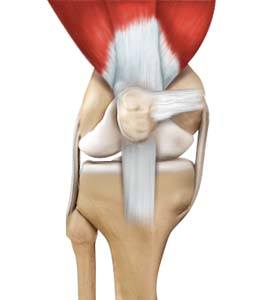
Medial Patellofemoral Ligament Anatomy
The medial patellofemoral ligament is a band of tissue that extends from the femoral medial epicondyle to the superior aspect of the patella. It is a major ligament that stabilizes the patella and helps in preventing patellar subluxation (partial dislocation) or dislocation.
Medial Patellofemoral Ligament Damage
The medial patellofemoral ligament can rupture or get damaged when there is patellar lateral dislocation. Dislocation can be caused by a direct blow to the knee, twisting injury to the lower leg, strong muscle contraction, or because of a congenital abnormality such as shallow or malformed joint surfaces.
What is Medial Patellofemoral Ligament Reconstruction?
Medial patellofemoral ligament reconstruction is a surgical procedure indicated for severe patellar instability.
Medial patellofemoral ligament reconstruction is performed by following the basic principles of ligament reconstruction such as:
- Graft selection: A strong and stiff graft should be selected.
- Location: The graft should be located isometrically.
- Correct tension: The tension set in the graft should be appropriate.
- Secure fixation: Stable fixation of the graft should be achieved.
- Avoid condylar rubbing or impingement: The graft should not rub against condyle or cause impingement.
Medial Patellofemoral Ligament Reconstruction Procedure
The procedure of medial patellofemoral ligament reconstruction involves the following steps:
Graft Selection and Harvest
Your surgeon will make a 4-6 cm skin incision over your knee, at the midpoint between the medial epicondyle and the medial aspect of the patella (kneecap). The underlying subcutaneous fat and fascia are cut apart to expose the adductor tendon. The tendon is then stripped using a tendon stripper and its free end is sutured. The diameter of the tendon graft is measured using a sizer.
Alternatively, a graft can be harvested from the quadriceps tendon.
Location of the Femoral Isometric Point
The graft should be placed isometrically to prevent it from overstretching and causing failure during joint movements. A transverse hole measuring 2.5 mm is made through the patella. Then a small incision is made over the lateral side of the patella and a strand of Vicryl suture material is inserted through the hole. Over this strand, a 2.5 mm Kirschner wire (K-wire) is passed and then inserted into the bone beside the medial epicondyle.
An instrument called pneumatic isometer is inserted into the hole made in the patella and the Vicryl isometric measurement suture material is also passed along. The knee is taken through its full range of motion and any changes in the length between the medial epicondylar K-wire and the medial aspect of the patella is recorded on the isometer. The position of the K-wire is adjusted until no deviations are read on the isometer during full range of motion. Once the isometric point is identified, a tunnel is drilled starting from the insertion of the adductor tendon until the isometric point is reached. The graft is pulled through this tunnel, then exits at the medial condyle and again passed through another tunnel that is made through the patella.
Correct Tension
The tension is set in the graft with your knee flexed up to 90° and the tension should be appropriate enough to control lateral excursion.
Secure Fixation
After bringing the tendon graft from the medial to the lateral side through the bone tunnel, it is turned onto the front surface of the patella where it is sutured.
Avoid Condylar Rubbing and Impingement
After graft fixation, the range of motion is checked to make sure there are no restrictions in the patellar or knee movements. The graft should not impinge or rub against the medial femoral condyle. If it is detected, the graft is suitably adjusted into proper position.
Postoperative Care after Medial Patellofemoral Ligament Reconstruction
A knee brace should be worn while walking for the first 3-6 weeks after surgery. Avoid climbing stairs, squatting and stretching your leg until there is adequate healing of the tendon. Rehabilitation exercises, continuous passive motion, and active exercises will be recommended.